Functions from these packages will be used throughout this document:
[R code]
library(conflicted) # check for conflicting function definitions# library(printr) # inserts help-file output into markdown outputlibrary(rmarkdown) # Convert R Markdown documents into a variety of formats.library(pander) # format tables for markdownlibrary(ggplot2) # graphicslibrary(ggfortify) # help with graphicslibrary(dplyr) # manipulate datalibrary(tibble) # `tibble`s extend `data.frame`slibrary(magrittr) # `%>%` and other additional piping toolslibrary(haven) # import Stata fileslibrary(knitr) # format R output for markdownlibrary(tidyr) # Tools to help to create tidy datalibrary(plotly) # interactive graphicslibrary(dobson) # datasets from Dobson and Barnett 2018library(parameters) # format model output tables for markdownlibrary(haven) # import Stata fileslibrary(latex2exp) # use LaTeX in R code (for figures and tables)library(fs) # filesystem path manipulationslibrary(survival) # survival analysislibrary(survminer) # survival analysis graphicslibrary(KMsurv) # datasets from Klein and Moeschbergerlibrary(parameters) # format model output tables forlibrary(webshot2) # convert interactive content to static for pdflibrary(forcats) # functions for categorical variables ("factors")library(stringr) # functions for dealing with stringslibrary(lubridate) # functions for dealing with dates and timeslibrary(broom) # Summarizes key information about statistical objects in tidy tibbleslibrary(broom.helpers) # Provides suite of functions to work with regression model 'broom::tidy()' tibbles
Here are some R settings I use in this document:
[R code]
rm(list =ls()) # delete any data that's already loaded into Rconflicts_prefer(dplyr::filter)ggplot2::theme_set( ggplot2::theme_bw() +# ggplot2::labs(col = "") + ggplot2::theme(legend.position ="bottom",text = ggplot2::element_text(size =12, family ="serif")))knitr::opts_chunk$set(message =FALSE)options('digits'=6)panderOptions("big.mark", ",")pander::panderOptions("table.emphasize.rownames", FALSE)pander::panderOptions("table.split.table", Inf)conflicts_prefer(dplyr::filter) # use the `filter()` function from dplyr() by defaultlegend_text_size =9run_graphs =TRUE
See also Hernán and Robins (2020) for a comprehensive treatment of causal inference from observational data.
1 Introduction
Regression models describe statistical associations between variables. But in many research settings, the goal is not merely to describe associations but to estimate causal effects: what would happen if we intervened to change a variable?
The causal inference framework covered in this chapter is based on the potential outcomes model (Rubin 1974; Holland 1986). This framework provides:
A precise language for defining causal effects
Explicit assumptions required to identify causal effects from data
Estimation methods that target specific causal estimands
The fundamental challenge in causal inference is that we can only observe one potential outcome for each unit: the outcome under the treatment that actually occurred. This is called the fundamental problem of causal inference(Holland 1986).
Definition 1 (Potential outcomes) For a binary treatment \(A \in \{0, 1\}\), the potential outcomes for unit \(i\) are:
\(Y_i(1)\): the outcome that would be observed if unit \(i\) received treatment (\(A_i = 1\))
\(Y_i(0)\): the outcome that would be observed if unit \(i\) received control (\(A_i = 0\))
These are also called counterfactual outcomes, because for each unit, one of them is necessarily counterfactual (it corresponds to a treatment that did not occur).
Definition 2 (Observed outcome) The observed outcome for unit \(i\) is the potential outcome corresponding to the treatment actually received: \[Y_i = Y_i(A_i) = A_i \cdot Y_i(1) + (1 - A_i) \cdot Y_i(0)\]
This is sometimes called the consistency assumption: the observed outcome under the observed treatment equals the potential outcome under that treatment.
Definition 3 (Individual causal effect) The individual causal effect for unit \(i\) is the difference between that unit’s two potential outcomes: \[\tau_i = Y_i(1) - Y_i(0)\]
Because of the fundamental problem of causal inference, we can never observe both \(Y_i(1)\) and \(Y_i(0)\) for the same unit, so individual causal effects are generally not identified.
3 Causal Estimands
Since individual causal effects are not identified, causal inference focuses on population-level causal estimands: averages of potential outcomes over a population.
Definition 4 (Average Treatment Effect (ATE)) The Average Treatment Effect is the expected difference in potential outcomes in the study population: \[\text{ATE} = \text{E}{\left[Y(1) - Y(0)\right]} = \text{E}{\left[Y(1)\right]} - \text{E}{\left[Y(0)\right]}\]
The ATE represents the average causal effect of treatment compared with control, averaged over all units in the population (both those who would and would not actually receive treatment).
Definition 5 (Average Treatment Effect on the Treated (ATT)) The Average Treatment Effect on the Treated is the expected difference in potential outcomes among units who actually received treatment: \[\text{ATT} = \text{E}{\left[Y(1) - Y(0) \mid A = 1\right]} = \text{E}{\left[Y(1) \mid A = 1\right]} - \text{E}{\left[Y(0) \mid A = 1\right]}\]
The ATT answers the question: “On average, how much did treatment help the people who received it?”
Definition 6 (Average Treatment Effect on the Untreated (ATU)) The Average Treatment Effect on the Untreated is the expected difference in potential outcomes among units who did not receive treatment: \[\text{ATU} = \text{E}{\left[Y(1) - Y(0) \mid A = 0\right]} = \text{E}{\left[Y(1) \mid A = 0\right]} - \text{E}{\left[Y(0) \mid A = 0\right]}\]
The ATU answers the question: “On average, how much would treatment have helped the people who did not receive it?”
4 Causal Assumptions
Three key assumptions are required to identify causal effects from observed data (Hernán and Robins 2020):
4.1 Consistency
Definition 7 (Consistency) The consistency assumption states that the observed outcome for a treated unit equals that unit’s potential outcome under treatment, and similarly for control: \[Y_i = Y_i(A_i)\]
Consistency requires that the treatment is well-defined: there is only one version of treatment, or different versions have the same effect on the outcome. Violations of consistency (e.g., different doses of a drug being lumped together as “treated”) can introduce bias.
4.2 Exchangeability (No Unmeasured Confounding)
Definition 8 (Exchangeability)Exchangeability (also called no unmeasured confounding or ignorability) states that, conditional on observed covariates \(\tilde{L}\), treatment assignment is independent of potential outcomes: \[A \perp\!\!\!\perp (Y(0), Y(1)) \mid \tilde{L}\]
Intuitively, this means that among individuals with the same covariate values, treatment was assigned as if at random — there are no unmeasured common causes of treatment and outcome.
Unconditional exchangeability (\(A \perp\!\!\!\perp (Y(0), Y(1))\)) holds in perfectly randomized trials. Conditional exchangeability requires adjusting for \(\tilde{L}\).
4.3 Positivity
Definition 9 (Positivity) The positivity assumption states that every individual has a positive probability of receiving each treatment level, conditional on their covariate values: \[0 < \text{P}{A = 1 \mid \tilde{L} = \tilde{l}} < 1
\quad \text{for all } \tilde{l} \text{ in the support of } \tilde{L}\]
Without positivity, some subgroups have no treated (or untreated) members, making it impossible to estimate the counterfactual outcome for those subgroups. This is sometimes called the positivity violation or practical positivity violation when near-zero probabilities occur in small strata.
5 Randomized Experiments
In a randomized controlled trial (RCT), treatment is assigned by the investigator using a random mechanism, independent of any characteristics of the participants. This makes the treatment groups exchangeable: the distribution of potential outcomes is the same in treated and untreated groups.
As a result, in a perfectly randomized trial:
\[\text{E}{\left[Y(1)\right]} = \text{E}{\left[Y \mid A = 1\right]}
\quad \text{and} \quad
\text{E}{\left[Y(0)\right]} = \text{E}{\left[Y \mid A = 0\right]}\]
The observed mean difference between treatment groups is an unbiased estimate of the ATE:
The “heart and estrogen/progestin study” (HERS) was a clinical trial of hormone therapy for prevention of recurrent heart attacks and death among 2,763 post-menopausal women with existing coronary heart disease (CHD) (Hulley et al. 1998).
The trial was conducted at 20 US clinical centers. Participants were randomized to receive either conjugated equine estrogens (0.625 mg/day) plus medroxyprogesterone acetate (2.5 mg/day) or a matching placebo (Hulley et al. 1998). Women were followed for an average of 4.1 years (Hulley et al. 1998).
The primary outcome was nonfatal myocardial infarction or CHD death (Hulley et al. 1998).
In HERS, hormone therapy (HT) was randomized, so the treatment groups were exchangeable at baseline. The observed difference in CHD event rates between the HT and placebo groups estimates the causal effect of HT.
Despite observational studies suggesting up to 35–80% fewer recurrent CHD events among hormone users than non-users, (Hulley et al. 1998), HERS found no significant difference in CHD event rates between the hormone therapy (HT) and placebo groups (relative hazard 0.99; 95% CI: 0.80–1.22) (Hulley et al. 1998).
The HERS investigators noted a statistically significant time trend: more CHD events occurred in the HT group in year 1, while fewer occurred in years 4 and 5, suggesting that HT may have early harmful effects that are later reversed.
A key finding was that HT significantly altered lipid profiles:
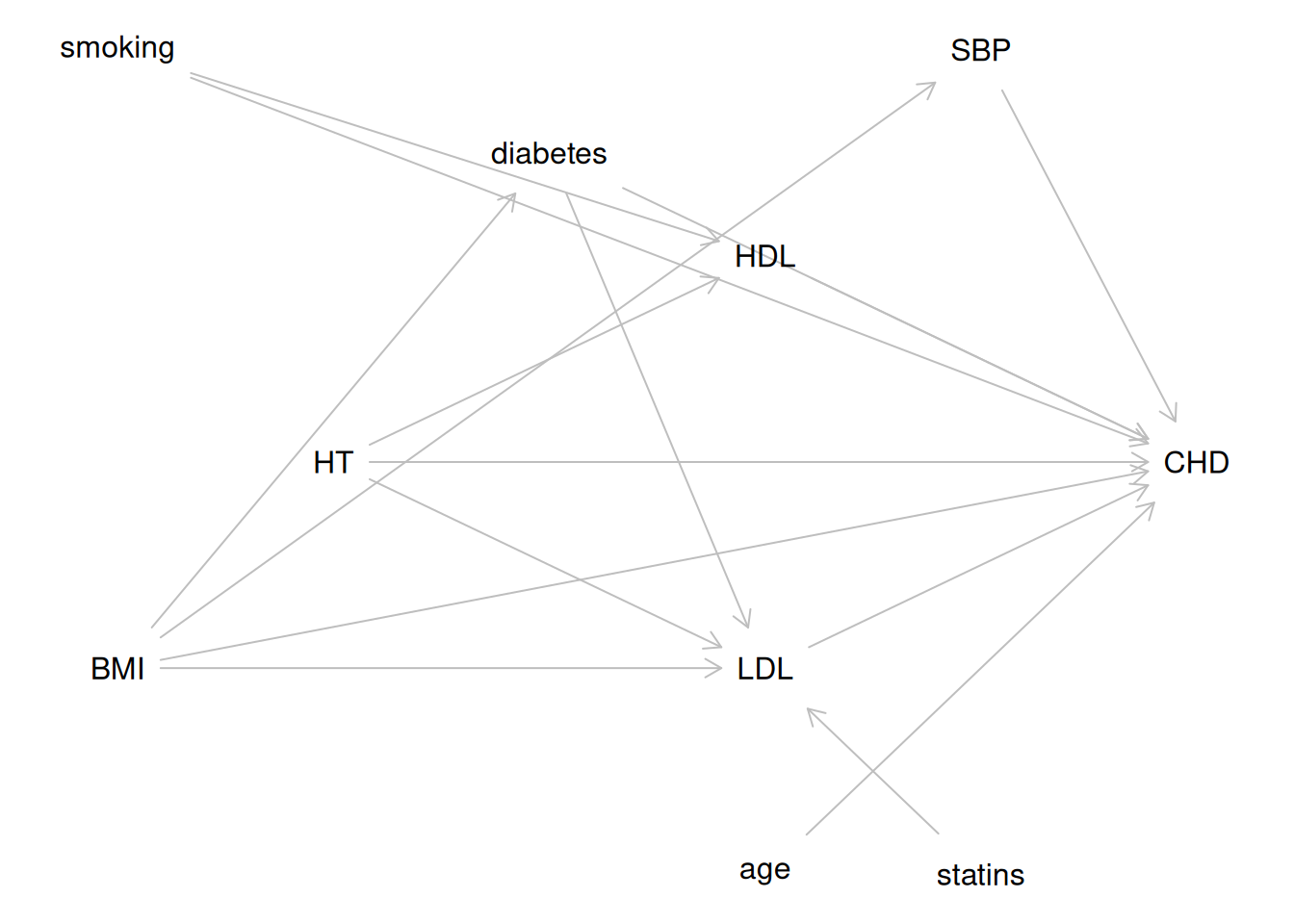
Yet these favorable lipid changes did not translate into fewer CHD events overall. One explanation consistent with the DAG in Figure 1 is that the effects of HT on lipids (a mediator pathway) were offset by other, harmful pathways — possibly thrombotic — that are not captured in the lipid mediators.
5.2 Covariate adjustment in RCTs
Although randomization ensures no confounding, adjusting for baseline covariates in an RCT can still be useful:
Improved precision: Adjusting for strong predictors of the outcome reduces residual variance and narrows confidence intervals.
Covariate imbalance: When randomization produces chance imbalances in small trials, adjustment can correct for these.
However, in an RCT, covariates that are mediators of the treatment effect (i.e., variables affected by treatment) should generally not be adjusted for when estimating the total causal effect of treatment. Adjusting for mediators blocks part of the causal pathway and gives only the direct effect of treatment.
6 Observational Studies
In an observational study, treatment is not assigned by the investigator. Instead, individuals self-select into treatment, or treatment is assigned based on clinical or administrative criteria. As a result, treatment groups may differ systematically in ways that also affect the outcome — this is called confounding.
6.1 Confounding
Definition 10 (Confounding)Confounding occurs when there is a common cause of both the treatment \(A\) and the outcome \(Y\). This common cause is called a confounder.
In the potential outcomes framework, confounding means that treatment assignment is not independent of potential outcomes: \[A \not\perp\!\!\!\perp (Y(0), Y(1))\]
As a result, the observed association between \(A\) and \(Y\) does not equal the causal effect of \(A\) on \(Y\).
Directed Acyclic Graphs (DAGs) provide a formal graphical tool for representing causal assumptions and identifying confounders, mediators, colliders, and sufficient adjustment sets.
6.2 Directed Acyclic Graphs (DAGs)
A Directed Acyclic Graph (DAG) is a graphical model that encodes assumed causal relationships among variables.
In a DAG:
Nodes represent variables.
Directed edges (arrows) represent direct causal effects.
The graph is acyclic: there are no directed cycles (a variable cannot cause itself, even indirectly).
DAGs are used in causal inference to:
Identify confounders that must be adjusted for.
Identify mediators that should generally not be adjusted for when estimating the total causal effect.
Identify colliders that should not be adjusted for (adjusting for a collider opens a non-causal path).
6.3 Key concepts from DAG theory
Definition 11 (Confounder) A confounder of the relationship between an exposure \(X\) and outcome \(Y\) is a variable \(C\) that is a common cause of both \(X\) and \(Y\). By contrast, a mediator lies on the causal path from \(X\) to \(Y\) and is not a common cause of \(X\) and \(Y\).
Adjusting for confounders removes confounding bias.
Definition 12 (Mediator) A mediator\(M\) is a variable that lies on the causal pathway from the exposure \(X\) to the outcome \(Y\): \[X \to M \to Y\]
Adjusting for a mediator blocks the indirect causal pathway through \(M\), so the estimated coefficient for \(X\) reflects only the direct effect of \(X\) on \(Y\) not through \(M\).
Whether to adjust for mediators depends on the research question:
If you want the total causal effect of \(X\) on \(Y\), do not adjust for \(M\).
If you want the direct effect of \(X\) on \(Y\) not through \(M\), adjust for \(M\).
Definition 13 (Collider) A collider is a variable \(L\) that is caused by two or more variables on a path: \[X \to L \leftarrow Y\]
Adjusting for a collider opens a non-causal (backdoor) path between \(X\) and \(Y\), introducing collider bias.
Definition 14 (Backdoor criterion) A set of variables \(\tilde{L}\) satisfies the backdoor criterion with respect to the ordered pair \((A, Y)\) in a DAG if:
No variable in \(\tilde{L}\) is a descendant of \(A\).
\(\tilde{L}\) blocks every path between \(A\) and \(Y\) that has an arrow into \(A\) (a “backdoor” path).
If \(\tilde{L}\) satisfies the backdoor criterion, then adjusting for \(\tilde{L}\) identifies the causal effect of \(A\) on \(Y\): \[\text{E}{\left[Y(a)\right]} = \sum_{\tilde{l}} \text{E}{\left[Y \mid A = a, \tilde{L} = \tilde{l}\right]} \text{P}{\tilde{L} = \tilde{l}}\]
6.4 HERS study DAG
The “heart and estrogen/progestin study” (HERS) was a clinical trial of hormone therapy for prevention of recurrent heart attacks and death among 2,763 post-menopausal women with existing coronary heart disease (CHD) (Hulley et al. 1998).
The trial was conducted at 20 US clinical centers. Participants were randomized to receive either conjugated equine estrogens (0.625 mg/day) plus medroxyprogesterone acetate (2.5 mg/day) or a matching placebo (Hulley et al. 1998). Women were followed for an average of 4.1 years (Hulley et al. 1998).
The primary outcome was nonfatal myocardial infarction or CHD death (Hulley et al. 1998).
We now examine the assumed causal structure among key baseline variables, treatment, and recurrent CHD events.
Figure 1 shows a DAG for the HERS study, representing the assumed causal structure among key variables.
The main goal of the HERS study was to estimate the causal effect of hormone therapy (HT) on recurrent CHD event risk.
Table 1
Data dictionary for key HERS variables used in the DAG and examples.
Variable
Meaning
Type
HT
Hormone-therapy assignment (placebo vs estrogen+progestin)
Table 3: Summary table for LDL analysis variables in HERS
Characteristic
Overall
N = 2,7521
Placebo
N = 1,3791
HT
N = 1,3731
LDL cholesterol (mg/dl)
141 (120, 166)
141 (119, 165)
141 (120, 167)
age in years
67 (62, 72)
68 (62, 72)
67 (62, 72)
BMI (kg/m^2)
27.7 (24.6, 31.7)
27.6 (24.5, 31.7)
27.9 (24.7, 31.8)
Unknown
5
4
1
diabetes
727 (26%)
350 (25%)
377 (27%)
smoking
355 (13%)
180 (13%)
175 (13%)
statins
998 (36%)
516 (37%)
482 (35%)
1 Median (Q1, Q3); n (%)
Unadjusted model
[R code]
model_ldl_unadj <-lm(LDL ~ HT, data = hers_ldl)model_ldl_unadj |>tbl_regression() |>bold_labels()
Table 4: Unadjusted linear regression for LDL in HERS
Characteristic
Beta
95% CI
p-value
HT
Placebo
—
—
HT
0.36
-2.5, 3.2
0.8
Abbreviation: CI = Confidence Interval
Adjusted model
Based on the DAG in Figure 1, BMI is a common cause of LDL and other outcomes (but age does not confound the HT → LDL relationship, since HT was randomized).
In a randomized trial, treatment assignment is independent of pre-treatment covariates, so confounding adjustment is not required to estimate the causal effect. However, adjusting for strong predictors of the outcome can improve precision.
[R code]
model_ldl_adj <-lm(LDL ~ HT + age + BMI + diabetes + statins, data = hers_ldl)model_ldl_adj |>tbl_regression() |>bold_labels()
Table 5: Adjusted linear regression for LDL in HERS
Characteristic
Beta
95% CI
p-value
HT
Placebo
—
—
HT
-0.14
-2.9, 2.6
>0.9
age in years
-0.23
-0.44, -0.02
0.035
BMI (kg/m^2)
0.46
0.19, 0.72
<0.001
diabetes
No
—
—
Yes
-4.6
-7.9, -1.4
0.005
statins
No
—
—
Yes
-17
-20, -14
<0.001
Abbreviation: CI = Confidence Interval
Note that statins is a strong predictor of LDL (statin medications are prescribed specifically to lower LDL). Including statins substantially reduces residual variability, improving precision of the HT coefficient.
6.7 An observational study example: WCGS
The HERS study is a randomized trial, so confounding of the treatment-outcome relationship is not a concern. To illustrate DAG-guided confounder selection in an observational study, we use the Western Collaborative Group Study (WCGS).
The WCGS was a prospective cohort study of 3,154 men employed by California companies, followed from 1960 to 1969 (Rosenman et al. 1975). The exposure of primary interest is Type A behavior pattern (a personality trait characterized by competitive drive, time urgency, and hostility), hypothesized to increase CHD risk independently of classic cardiovascular risk factors.
Table 6
Data dictionary for key WCGS variables used in the DAG and examples.
Variable
Meaning
Type
personality_type
Personality type (Type A vs Type B behavior pattern)
Binary categorical
CHD
Coronary heart disease event outcome
Binary categorical
age
Baseline age (years)
Continuous
smoking
Baseline smoking status
Binary categorical
chol
Serum cholesterol
Continuous
sbp
Systolic blood pressure
Continuous
bmi
Body mass index
Continuous
[R code]
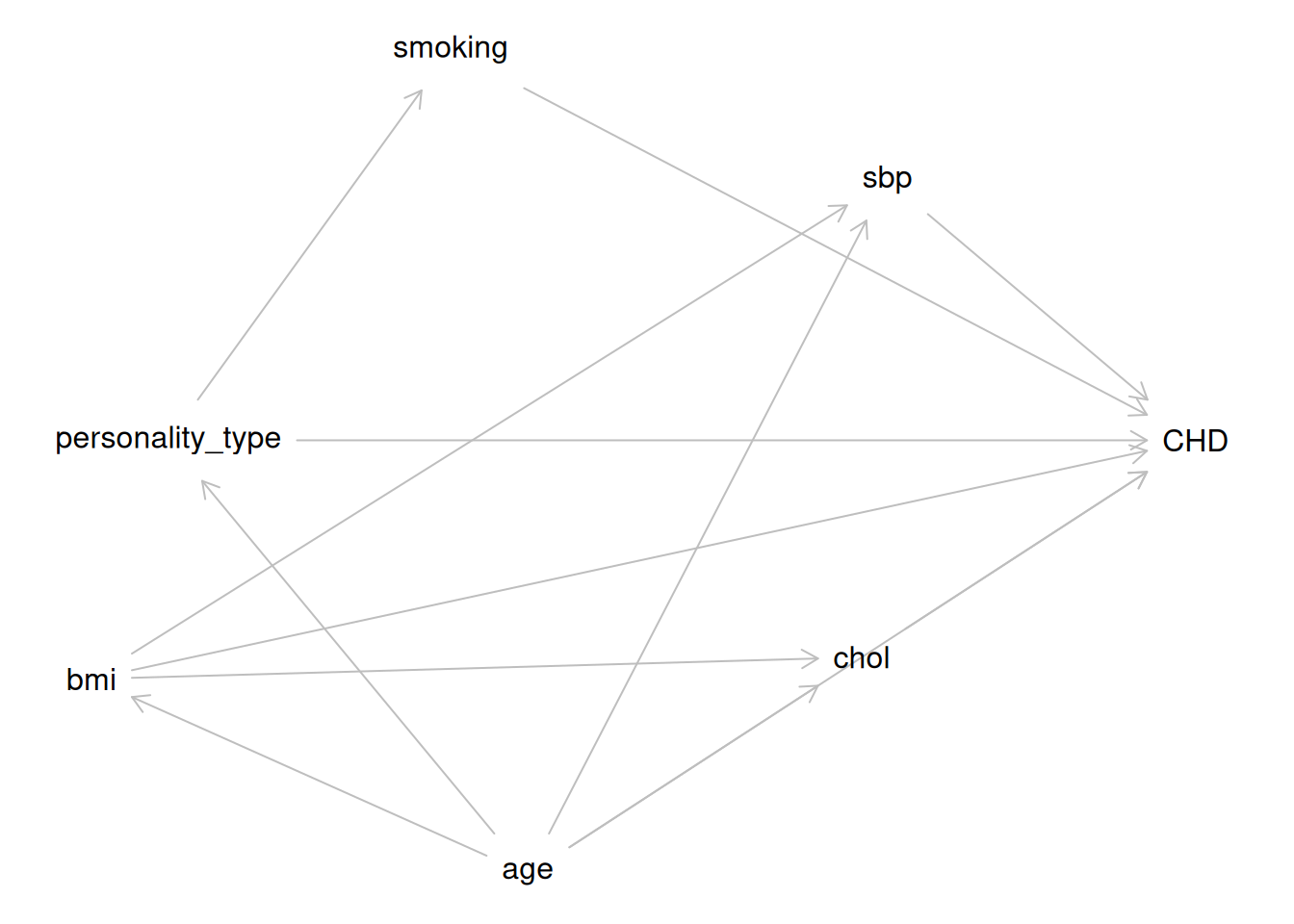
wcgs_dag <-dagitty('dag { personality_type [exposure, pos="0,0"] CHD [outcome, pos="4,0"] age [pos="1.4,2"] bmi [pos="-0.3,1.1"] smoking [pos="1.1,-1.8"] chol [pos="2.7,1"] sbp [pos="2.8,-1.2"] personality_type -> CHD age -> CHD age -> chol age -> sbp age -> bmi age -> personality_type personality_type -> smoking smoking -> CHD chol -> CHD sbp -> CHD bmi -> CHD bmi -> chol bmi -> sbp }')plot(wcgs_dag)
Figure 2: Directed Acyclic Graph (DAG) for the WCGS study. personality_type = personality type (exposure; Type A vs Type B); CHD = coronary heart disease events (outcome); chol = serum cholesterol; sbp = systolic blood pressure.
In Figure 2, age is a confounder: it has direct causal arrows to both the exposure (personality_type) and the outcome (CHD). We assume personality_type -> smoking rather than smoking -> personality_type as an explicit modeling assumption for this teaching example: we treat Type A behavior pattern as a relatively stable trait that can influence smoking behavior. Under that assumption, smoking is a mediator on the path personality_type -> smoking -> CHD, not a confounder. BMI is causally affected by age. Cholesterol and SBP are causally affected by both age and BMI. All three have direct effects on CHD. Unlike in HERS, where HT was randomized to estimate its causal effect on CHD event risk, we cannot assume the exposure is unconfounded here.
[R code]
wcgs_adj <-adjustmentSets( wcgs_dag,exposure ="personality_type",outcome ="CHD",type ="minimal")wcgs_adj#> { age }
7 Regression Adjustment
Under the causal assumptions (consistency, conditional exchangeability, and positivity), the causal effect can be estimated by adjusting for the confounders \(\tilde{L}\) in a regression model.
7.1 Direct standardization (G-computation)
The G-computation estimator (also called direct standardization or standardization) estimates the ATE by:
Fitting a regression model: \(\hat{\mu}(a, \tilde{l}) = \widehat{\text{E}{\left[Y \mid A = a, \tilde{L} = \tilde{l}\right]}}\)
Predicting the potential outcome mean for each individual under both treatment levels \(a = 1\) and \(a = 0\): \[\hat{Y}_i(a) = \hat{\mu}(a, \tilde{L}_i)\]
Averaging over the study population: \[\widehat{\text{E}{\left[Y(a)\right]}} = \frac{1}{n} \sum_{i=1}^n \hat{Y}_i(a)\]
Estimating the ATE as the contrast: \[\widehat{\text{ATE}} = \widehat{\text{E}{\left[Y(1)\right]}} - \widehat{\text{E}{\left[Y(0)\right]}}\]
7.2 Regression adjustment in linear models
When the outcome is continuous and the regression model is linear, G-computation simplifies to the adjusted treatment coefficient from a linear regression:
Under consistency, conditional exchangeability, and positivity, the coefficient \(\beta_A\) estimates the average causal effect of \(A\) on \(Y\) (the ATE, if the model is correctly specified and effect modification by \(\tilde{L}\) is absent).
7.3 Example: regression adjustment for LDL in HERS
The HERS study DAG (see Section 6.4) shows that LDL and HDL are mediators of the HT → CHD pathway. For estimating the total causal effect of HT on CHD, we should not adjust for LDL or HDL.
However, to estimate the causal effect of HT on LDL itself, we use a separate regression model with LDL as the outcome. In this model, LDL is no longer a mediator but the outcome of interest.
Since HT was randomized in HERS, no adjustment is needed for causal identification of HT → LDL. However, adjusting for strong predictors of LDL improves precision:
library(gtsummary)model_ldl_adj <-lm(LDL ~ HT + age + BMI + diabetes + statins, data = hers_ldl)model_ldl_adj |>tbl_regression() |>bold_labels()
Table 7: Adjusted regression for the causal effect of HT on LDL in HERS. Since HT was randomized, adjustment is for precision only.
Characteristic
Beta
95% CI
p-value
HT
Placebo
—
—
HT
-0.14
-2.9, 2.6
>0.9
age in years
-0.23
-0.44, -0.02
0.035
BMI (kg/m^2)
0.46
0.19, 0.72
<0.001
diabetes
No
—
—
Yes
-4.6
-7.9, -1.4
0.005
statins
No
—
—
Yes
-17
-20, -14
<0.001
Abbreviation: CI = Confidence Interval
The estimated causal effect of HT on LDL is approximately −11 mg/dL (negative = lower LDL on HT), with narrower confidence intervals than the unadjusted estimate.
8 Propensity Score Methods
Propensity score methods are an alternative approach to confounding adjustment in observational studies. They replace adjustment for a high-dimensional confounder set \(\tilde{L}\) with adjustment for a single scalar summary: the propensity score.
Definition 15 (Propensity score) The propensity score is the conditional probability of treatment given the observed covariates: \[e(\tilde{L}) = \text{P}{A = 1 \mid \tilde{L}}\]
Rosenbaum and Rubin (1983) showed that if \(A \perp\!\!\!\perp (Y(0), Y(1)) \mid \tilde{L}\) (conditional exchangeability given \(\tilde{L}\)), then also: \[A \perp\!\!\!\perp (Y(0), Y(1)) \mid e(\tilde{L})\]
That is, the propensity score is a balancing score: conditioning on the propensity score is sufficient to remove confounding.
8.1 Propensity score estimation
The propensity score is estimated by fitting a model for the probability of treatment given covariates, typically using logistic regression:
The estimated propensity score \(\hat{e}(\tilde{L}_i)\) is the predicted probability of treatment for each individual.
8.2 Propensity score methods
There are four main ways to use the propensity score:
Matching: Match each treated individual to one or more untreated individuals with similar propensity scores. The matched dataset is then analyzed as a simple comparison.
Stratification (subclassification): Divide individuals into strata based on propensity score quantiles. Estimate the causal effect within each stratum, then combine across strata.
Inverse probability weighting (IPW): Weight each individual by the inverse of their probability of receiving the treatment they actually received. See Definition 16 below.
Covariate adjustment using the propensity score: Include the estimated propensity score as a covariate in a regression model for the outcome.
Definition 16 (Inverse probability weighting (IPW)) The inverse probability weighted (IPW) estimator of the ATE uses weights: \[w_i = \frac{A_i}{\hat{e}(\tilde{L}_i)} +
\frac{1 - A_i}{1 - \hat{e}(\tilde{L}_i)}\]
The IPW estimator of \(\text{E}{\left[Y(a)\right]}\) is: \[\widehat{\text{E}{\left[Y(a)\right]}}_{\text{IPW}} =
\frac{\sum_{i: A_i = a} w_i Y_i}{\sum_{i: A_i = a} w_i}\]
Reweighting by \(w_i\) creates a pseudo-population in which treatment is independent of covariates, effectively removing confounding.
8.3 Propensity score example: WCGS
In the WCGS study, we can use propensity score methods to estimate the causal effect of Type A behavior on CHD. We first fit a logistic regression model predicting Type A behavior from the confounders identified by the DAG (Section 6.7):
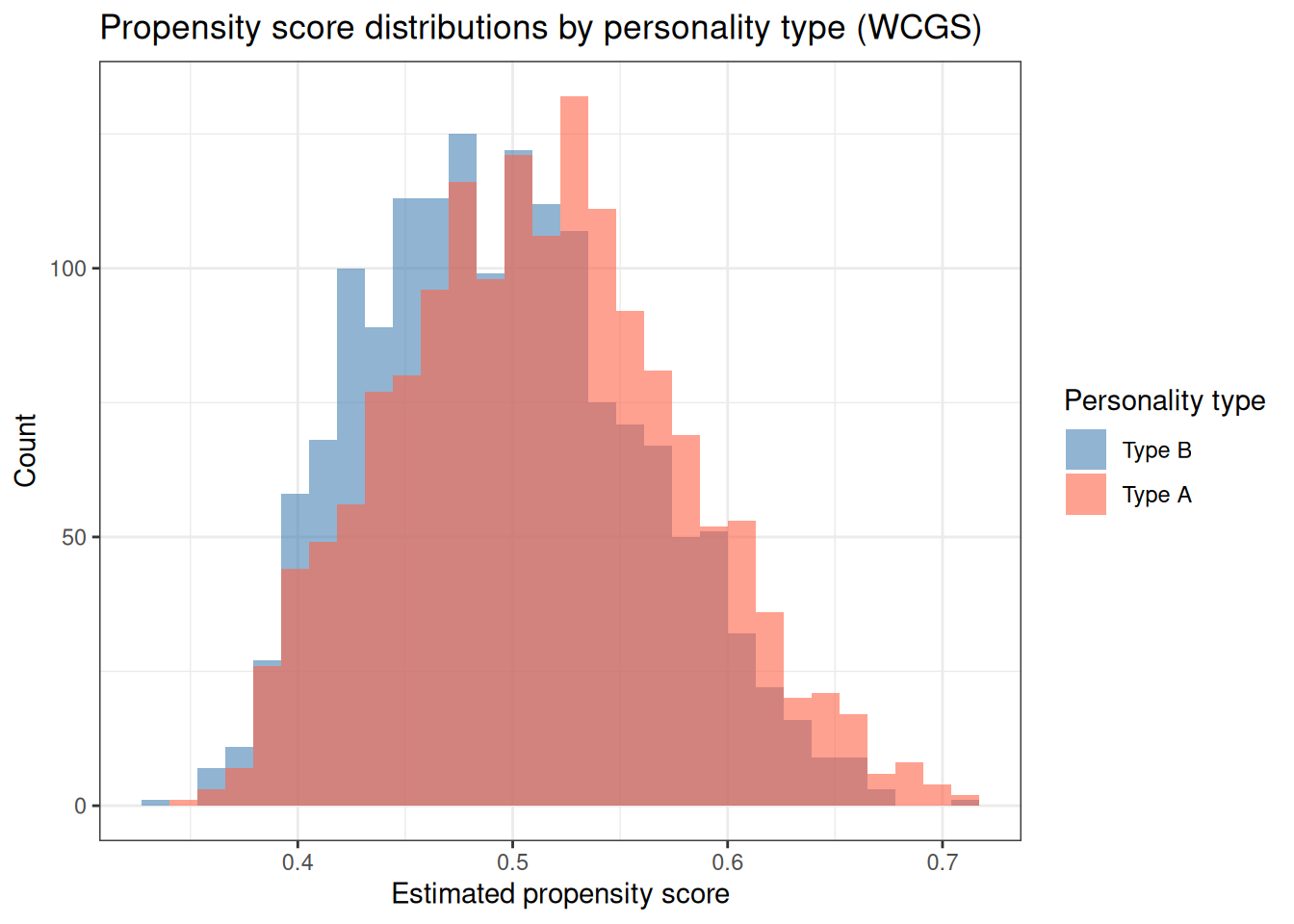
library(ggplot2)ggplot(wcgs_ps, aes(x = ps, fill =factor(dibpat_A))) +geom_histogram(alpha =0.6, bins =30, position ="identity") +scale_fill_manual(values =c("steelblue", "tomato"),labels =c("Type B", "Type A"),name ="Personality type" ) +labs(x ="Estimated propensity score",y ="Count",title ="Propensity score distributions by personality type (WCGS)" ) +theme_bw()
Figure 3: Distribution of estimated propensity scores by personality type in the WCGS study. Good overlap between the two groups (the overlap or common support assumption) supports positivity.
Abbreviations: CI = Confidence Interval, OR = Odds Ratio
9 Summary
Causal inference requires moving beyond statistical association to make statements about what would happen under intervention. The key ideas from this chapter are:
Potential outcomes define what we mean by a causal effect. For each unit, there is a potential outcome under treatment and a potential outcome under control; the individual causal effect is their difference.
Causal estimands — ATE, ATT, ATU — summarize the causal effect at the population level.
Three key assumptions are needed to identify causal effects from observed data:
Consistency: The observed outcome equals the potential outcome under the received treatment.
Exchangeability: Treatment assignment is independent of potential outcomes, given measured confounders.
Positivity: Every individual has a positive probability of receiving each treatment level.
Randomized experiments achieve unconditional exchangeability and allow unbiased causal inference from simple treatment comparisons.
In observational studies, confounding violates exchangeability. DAGs help identify which variables are confounders, mediators, and colliders, and the backdoor criterion identifies sufficient adjustment sets.
Estimation methods — regression adjustment (G-computation) and propensity score methods (matching, stratification, IPW) — can recover causal estimates under the three assumptions above.
Learning Objectives
After completing this chapter, students should be able to:
Define potential outcomes and the fundamental problem of causal inference.
Distinguish the ATE, ATT, and ATU, and explain when they agree and when they differ.
State and interpret the three core causal assumptions: consistency, exchangeability, and positivity.
Use a DAG to identify confounders, mediators, and colliders, and apply the backdoor criterion to select sufficient adjustment sets.
Describe the G-computation estimator and explain how it relates to regression adjustment.
Describe propensity score methods (matching, stratification, IPW) and explain how they use the propensity score to remove confounding.
Contrast causal inference from randomized trials with causal inference from observational studies, and articulate the additional assumptions required in each setting.
Holland, Paul W. 1986. “Statistics and Causal Inference.”Journal of the American Statistical Association 81 (396): 945–60. https://doi.org/10.2307/2289064.
Hulley, Stephen, Deborah Grady, Trudy Bush, et al. 1998. “Randomized Trial of Estrogen Plus Progestin for Secondary Prevention of Coronary Heart Disease in Postmenopausal Women.”JAMA : The Journal of the American Medical Association (Chicago, IL) 280 (7): 605–13.
Rosenbaum, Paul R., and Donald B. Rubin. 1983. “The Central Role of the Propensity Score in Observational Studies for Causal Effects.”Biometrika 70 (1): 41–55. https://doi.org/10.1093/biomet/70.1.41.
Rosenman, Ray H, Richard J Brand, C David Jenkins, Meyer Friedman, Reuben Straus, and Moses Wurm. 1975. “Coronary Heart Disease in the Western Collaborative Group Study: Final Follow-up Experience of 8 1/2 Years.”JAMA 233 (8): 872–77. https://doi.org/10.1001/jama.1975.03260080034016.
Rubin, Donald B. 1974. “Estimating Causal Effects of Treatments in Randomized and Nonrandomized Studies.”Journal of Educational Psychology 66 (5): 688–701. https://doi.org/10.1037/h0037350.
Vittinghoff, Eric, David V Glidden, Stephen C Shiboski, and Charles E McCulloch. 2012. Regression Methods in Biostatistics: Linear, Logistic, Survival, and Repeated Measures Models. 2nd ed. Springer. https://doi.org/10.1007/978-1-4614-1353-0.